A
Cancer Pain Tutorial
A
Comprehensive Visual Short Course
on Cancer Pain Management
|
|
|
| Nerve
Compression or Infiltration |
|
|
Pain
Type : Nociceptive Neuropathic
Psychogenic
|
|
Cause: Tumor
Invasion
of:
- Intercostals Spaces
- Paravertebral Spaces
- Retroperitoneal Spaces
|
|
Symptoms:
Due
to Peripheral Nerve Involvement:
- Constant burning pain
with dysesthesia.
- Pain is radicular and
usually unilateral
|
| Diagnosis:
CT Scanning Most Useful
Diagnostic Tool |
Involvement due to nerve
compression or infiltration is most commonly seen by tumors which
invade the intercostal, the paravertebral or the retroperitoneal spaces.
Symptoms of peripheral
nerve involvement: Constant burning pain with dysesthesia. in an area
of sensory loss. Pain is radicular and usually unilateral. Documentation
of the entrapped nerve can be done using CT scanning of the anatomic
region of nerve compression.
|
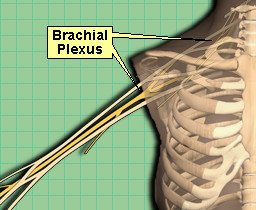
| Brachial
Plexopathy |
|
Pain
Type : Nociceptive Neuropathic Psychogenic |
|
Cause:
Direct Infiltration or Compression Upon the Nerve By Tumor or Metastasis
|
|
Effects:
Burning, Tingling Numbing in 95% of Patients
Neurological Findings : Weakness, Atrophy of Hand Muscles, Horner's
Syndrome, (ptosis, miosis, anhidrosis)
|
| Diagnosis: CT
Scanning Most Useful Diagnostic Tool |
Pain
is the initial symptom in 95% of patients with Brachial plexopathy
.
The most
common neurological findings are weakness and atrophy of hand muscles.
With upper brachial plexus involvement the thumb and index finger
are most commonly involved. In the lower brachial plexus, the 4th
and 5th fingers are usually involved. HornerÕs Syndrome (ptosis,
miosis, anhidrosis) is common.
Pain can
be caused by radiation fibrosis, as well as tumor. The common distinguishing
factor being: neurological signs precede onset of pain when the etiology
is radiation fibrosis. CT scanning is the most useful diagnostic
tool in assessment of this syndrome. |
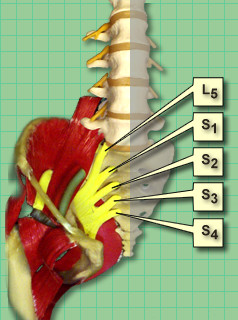
| Lumbosacral
Plexopathy |
|
|
Pain
Type : Nociceptive Neuropathic Psychogenic |
| Associated
Cancers: Prostate, Testicle, Rectum, Bladder, Cervix |
|
Cause:
Direct Infiltration or Compression Upon the Nerve By Tumor or Metastasis
|
|
Effects:
Constant Dull, Aching, Pressure-Like Sensation In Hip or Sacral Areas. Occasional
Sensation of Burning.
Neurological Findings :
Lower Plexus: Foot Drop, Pelvic Lordosis,
Numbness of Thigh, Sole, and Perineum.
Upper Plexus: Motor loss is manifested by flexor
weakness with difficulty negotiating stairs. Sensory loss is most
often numbness in anterior thigh.
|
Diagnosis: CT
Scanning Most Useful Diagnostic Tool
Differential
Diagnosis : Aortic Aneurysm, Diabetes, Trauma, Lumbosacral
Neuritis |
Lumbosacral
plexopathy is seen in patients with locally extensive cancers of
the prostate, testicle, rectum, bladder or cervix.
Pain is
usually the first symptom of plexus involvement, followed weeks later
by sensory and motor loss in the lower extremity. This pain us a
constant dull, aching, pressure-like sensation in the hip or sacral
areas with only occasional sensations of burning pain in those areas.
Incontinence is associated only about 10% of the time.
The lower
part of the plexus is most often involved. The nerve roots L5 to
S3 are the most common nerve roots involved. Most common clinical
signs are foot drop, pelvic lordosis. Numbness of the thigh, the
sole of the foot, and perineum.
The upper
plexus can also be invaded by tumor. Motor loss is manifested by
flexor weakness with difficulty in negotiating stairs. Sensory loss
is most often numbness in the anterior high.
Differential
Diagnosis:
- Aortic
aneurysm
- Diabetes
mellitus
- Trauma
- Lumbosacral
neuritis
|
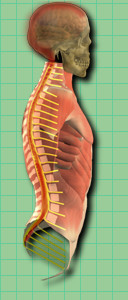
| Leptomeningeal
Metastasis |
|
Pain
Type : Nociceptive Neuropathic Psychogenic |
| Associated
Cancers: Prostate, Testicle, Rectum, Bladder, Cervix |
|
Cause:
Direct Infiltration or Compression Upon the Nerve By Tumor or Metastasis
|
|
Effects:
Burning, Tingling Numbing in 95% of Patients.
Neurological Findings: Weakness, Atrophy
of Hand Muscles, Horner's
Syndrome, (ptosis, miosis, anhidrosis)
|
| Diagnosis: Lumbar
Puncture, Elevated
CSF Protein and Low Glucose, MRI
often shows increased signal in the meninges. |
Pain
occurs in 40% of patients who have Leptomeningeal disease. Headache
without neck stiffness is a common finding.
Low back
pain and vomiting are frequent complaints. Patients often present
with cognitive failure (somnolence, mental confusion) and cranial
nerve involvement.
The best
way to make a diagnosis is a lumbar puncture to recover malignant
cells from the spinal fluid. Elevated cerebrospinal fluid protein
and low glucose concentrations are frequently associated with this
syndrome. MRI with gadolinium contrast frequently shows increased
signal in the meninges.
|